
To Give Birth In A New Country/Culture

To Give Birth In A New Country/Culture; The Challenges And Maternal Healthcare Systems in different countries
Author: Philomena Okyere, Bsc student, Bachelor of healthcare, Nursing, Novia UAS.
Supervisor: Anita Wikberg, RN. RM. PhD, Senior Lecturer, Novia UAS.
ABSTRCT
Childbirth is essential event in human lives and it involves physical, mental, emotional, social, and cultural needs. This life event does not matter the geographical location of a person or a group of persons. For this matter, evidence available suggests that the number of babies born to foreigners are on the rise in almost all developed countries. The reasons for this development include, family reunion marriages, political stabilities, good maternal health care system, good policies and studies. Despite these opportunities in healthcare system in some developed countries, maternal mortality rate among foreigners continue to be higher as compared to the local people around the developed world. On this note, the researcher analyzed various literatures on maternal healthcare in different countries and the challenges faced by foreigners in childbirth. The key findings from this study are, unfavourable healthcare policies for foreigner, language and communication barrial, cultural difference and beliefs, insufficient knowledge of the use of maternal services and finally, the cost of maternal healthcare in some developed countries.
_______________________________________________________________________________
Language: English
Key Words: childbirth, migrants, challenges, new country.
Introduction
Global migration has been a key factor among foreign affairs due to the fast rising economic, social, and cultural impact in origin and host countries. This has been an important issue of the recent world economy. Among every 35 people of the world’s population, 3 percent are found to be immigrants. A lot of people especially from developing countries are seeking for good opportunities abroad because of political instabilities, some also come, through marriage, and as students (Schiff, 2007, p8). According to the Guardian News (2020), more than 66,000 Americans gave birth in other countries where maternal cost was less expensive in 2019 to avoid the crushing financial and cost of starting family in the United States, and the high perinatal and maternal mortality in the USA.
In addition, due to issues such as wars, deteriorating security and lack of humanitarian conditions, migrant women relocate to developed countries to build their family or have better future for their children, for example gaining citizenship for their children. According to the Canadian Citizenship Act, all children born in Canada apart from foreign diplomat’s children are automatically Canadian citizens. However, at the same time one could experience stress from cultural shock, strife between hopes and possibilities, not getting a good job, and some migrants may experience post-traumatic stress disorders (Hill, Hunt, & Hyrkäs, 2012).
Also, migrant women are more often multiparity and are at risk of pregnancy and birth complications, which may affect them and their babies. Therefore, several social, psychological, cultural, physical, emotional, financial, and biological factors need to be considered during time of conception and childbirth (Miele, 2021; Malin; Ayers & Ford 2007, & Gissler, 2009).
The period right after childbirth to the sixth week after birth is known as puerperium. Problems that may arise during puerperium period may include, stillbirth, pelvic floor disorders, faecal incontinence, posttraumatic stress disorders, and maternal dissatisfaction. Due to the high maternal mortality among mothers in a foreign country, it is of importance to discuss about the challenges immigrants go through to give birth in a new country.
Culture differences
According to the World Health Organization (2022), quality healthcare should be safe, effective, person-centred, efficient, equitable and should bring a useful result, therefore, to achieve this, patients or client’s culture and cost of healthcare are some of the key elements to achieve this quality healthcare. Moreover, in every country, the way of living or culture is very important to the people in all aspects, and regarding pregnancy and childbirth, culture cannot be eliminated. To provide a quality care, it is important to know the individual differences, preferences and the people’s presumptions for pregnancy and giving birth, but in a case of being in a new country, health workers mostly do not know much about the foreigners as compared to the native people, and these usually results into poor prognosis.
Furthermore, women, especially Somalia women often complained of inappropriate care, pertaining to their female genital mutilation such as, inappropriate touching of their genital area during vaginal examination, Women who have past female genital mutilation are often immigrants, and they usually find themselves in countries where female genital mutilation is not practiced or not common, and healthcare workers do not have knowledge on how to help these women in times of pregnancy and labour (Chalmers, B. Omer-Hashi, K, 2002). Female genital mutilation is the part or whole removal of the female external genitalia or other injury to the female genital organs for non-medical purposes (WHO, 2022). Women with female genital mutilation are most of the time considered for caesarean birth and given pain medication which is against their will and culture (Chalmers, B. Omer-Hashi, K, 2002).
In addition, a result from a study in the United States about Somalia pregnant refugees showed that, insufficient knowledge about practices, culture and needs of Somalia pregnant refugees served as a hindrance in providing good quality care (Hill, Hunt, & Hyrkäs, 2012). Also, foreign women who do not have insurance mostly suffer to get sufficient prenatal care, they do not usually get early prenatal care for example, laboratory tests, follow ups, and when this happens, there could be complications such as stillbirth, preterm delivery, or low birth-rate or in a worst case, maternal death (Jarvis, D’Souza, Graves, 2019). Moreover, a study by Blais, and Maiga (1999), proved that, in a culturally diverse country such as United states, Canada and the United Kingdom, foreigners often access healthcare services less frequently or do not complete their care as required compared to the citizens.
Communication
For health professional to achieve patient satisfaction, and effective care, it is important to establish good patient to nurse relationship, effective communication, and trust (Chichire, & Purcărea, 2018). A study in Norway showed that women from India, and Canada expressed the dissatisfaction of not being involved in decision making, the women did not know what health professionals were doing for them, all they saw was being taken for procedures and this caused fear and panic to these women (Mehrara, Karine, Gjernes, & Young, 2022).
Poor communication skills in health care makes pregnant mothers feel worthless, less confident, and unmotivated to access healthcare. Not forgetting the language barriers, it makes it difficult for foreigners to access information and resources about maternity care and health care in general leading to disappointments and sadness (Malin, & Gissler, 2009). A study by Chichirez, and Purcărea, (2018), shows that, women who were not able to understand information given by healthcare professionals ended up seeking information from their home country.
Another study about Romanian women seeking maternal healthcare in Balkans, revealed that there was a miscommunication between doctors and clients, where doctors do not hear what clients say, neither nor clients hear what doctors say (Janevic, Sripad, Bradley, & Dimitrievska, 2011). In some countries one could get access to interpreters, but this is not guaranteed in all cases. However, one could find it very uncomfortable to share sensitive information with interpreters. Also, language barrier has shown to be the reason why most women are not motivated to attend antenatal care (Higginbottom, Morgan, Alexandre, Chiu, Forgeron, et a., 2015).
Racism
Racism is derived from the word race, and it refers to a group of people with same physical characteristics, same ancestors and coming from same native land. Racism therefore is the discrimination or prejudice against a person based on their native origin or ethnicity and physical appearance for example, black colour is considered as having some common characteristics like, lower intelligence (Montreal, 2011). According to study by Janevic, et al (2011), three types of racism were found in maternal healthcare thus personally mediated racism, internalized racism, and institutional racism. Personally mediated racism where foreign mothers are treated differently from native women, the less educated being treated with no respect or doctors felt they do not obey instructions.
Also, internalised racism where mothers become guilty and blames themselves for what they are going through, some feeling low self-esteem because of the bad treatment. Institutional racism in the sense that foreigners are not considered when making a policy regarding maternal health or health in general for example restricting visitors or number of visitors or the number of people to be with pregnant woman during delivery, not attending to cultural needs, failure to educate foreigner on the right to health treatment, and cost of maternal healthcare in some countries. Some foreign women barely know the hospital’s policies concerning maternal health care (Janevic. et al, 2011)
Knowledge and use of maternity services
A person’s belief in health, diseases, and knowledge about health can influence their help-seeking attitude (Malin, & Gissler, 2009). Most foreigners from the developing countries do not know about western medicalized pregnancy. They mostly depend on their traditional medicine or having old people who already have the experience of childbirth to take care of them, so giving birth in a foreign country where they mostly use medical knowledge become difficult for them.
Moreover, some pregnant women in a new county have no knowledge about antenatal clinics nor the need to visit one, as they are not used to it. The women belief that their God will protect them and their babies more than going to the hospital. Some foreign women even belief that C-section is dangerous for the mother, and their child’s fertility in future, could be affected (Hill, et al, 2012).
It is important for healthcare worker to know about the pregnant woman, to rule out any existing medical conditions such as hypertension or diabetes or to detect any complications for an early intervention, but if this is not the case, then it becomes a problem for healthcare workers during childbirth and the probability of these pregnant women getting complications is high.
Comparing Finland and United States Maternal healthcare systems
United States
In the United States childbirth is organized in the homes, birth centres and the hospitals. Maternal care is paid, and the cost varies according to the services and quality of services one requires thus one’s maternal healthcare may be influenced by state policies and financial status. Maternal healthcare in the United States is quite distinctive from many nations for these reasons, most of the hospital births are attended by physicians thus (90.6%) with few hospital births conducted by certified nurse midwives (8.7%) and birth attendances may vary depending on one’s status (National Academies of Sciences et al., 2020).
Moreover, hospitals have different practices, and this can affect care provided from one hospital to the other, for example number of birth attendance may vary, value and culture may differ for instance, there could be policies that, after one caesarean birth one may not have normal delivery for the subsequent babies. According to a study by Triebwasser, Kamdar, Moniz, and Langen (2018), about 43.2% of hospitals did not have vaginal delivery after caesarean birth from 2009 to 2015. Furthermore, United States have four levels (I -IV) of maternal care, thus basic care, special care, sub special care and regional perinatal healthcare respectively. Qualification for each type of care depends on resources and type of pregnancy. High risk pregnancies are treated at the fourth level. These levels of care were aimed for easy admission and transfer of clients with pregnancy related complication to promote maternal healthcare (American College of Obstetricians and Gynaecologists, 2019).
Maternal care is not universal thereby affecting the type of care women receives. Also, the cost of maternal care is expensive with average of $18,865 per birth. People usually buy private insurance to help pay their bills, but this may not cover for all costs. Additionally, Medicaid is an insurance system for the state and federal cooperation, that support the poor and the needy who are qualified, the qualification criteria depend on the women’s income. Undocumented immigrants do not qualify for the Medicaid insurance (Garfield, Orgera, Damico, 2019).
Also, United States have one of the highest maternal mortalities despite adopting the Millennium Development Goals, according to OECD report, maternal mortality in the U.S has increased to 17.4/100,000 birth in 2018 as compared to 1999 which was 9.9 /100,000 births. U.S born blacks has the highest maternal mortality rate followed by foreigners or immigrant women, and white Americans having the lowest maternal mortality rate. Furthermore, pregnant mothers who were unmarried, the less educated and those with age above 40 were affected most (Singh, 2021). According to various studies American women have the worst experiences of maternal healthcare as compared to countries like Sweden, Finland, Australia, New Zealand, Norway, Canada, and the Netherlands.
Fertility rate of foreigners in the United States
Fertility rate refers to the average number of children a woman can give birth to, in her lifetime. According to studies immigrant women from diaspora root have high fertility rate than non- Hispanic white women in the United State. For example, in 2001, there were about four million new births in the United State, and the fertility rate was about 2.1 birth per woman. Women from foreign origin, contributed to about 42 percent of the 2.1 birth per woman even though their population was 32 percent (PRB, 2003).
Figure 1 below shows the fertility rate in the United States of America 2019 and 2020. The graph elaborates the fertility rate of foreigners or migrants of all races, including, Spanish (Hispanic) and non-Spanish (Non-Hispanic) speaking women. The age specific fertility rate used was between 15-44 years. The graph shows migrants women has a high fertility rate as compared to the natives. However, although foreigners have high fertility rate than the local people, they usually have the worst outcome such as high perinatal mortality, caesarean birth, and low birth weight.
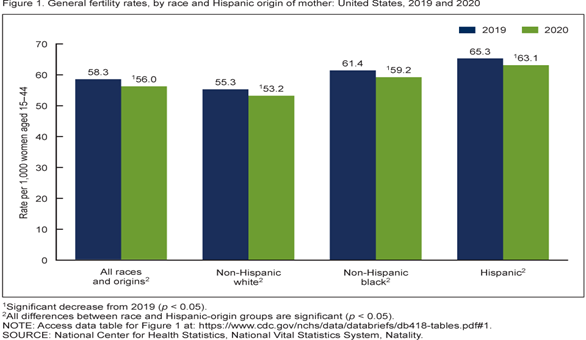
Source; National Center for Health Statistics (2021).
Finland
Finland has one of the best healthcare systems for pregnant women and children. Packages including parental leaves, child support and maternity leaves, the quality of the health care system attracts pregnant women to access maternal care more frequently (Malin, & Gissler, 2009). If a woman is a resident from EU or EEA country, Switzerland, UK, or Australia, the woman can receive care needed by pregnancy and childbirth, if only you are covered by the health insurance in their EU country and will have same fees as residents of Finland, but non-residents may have to pay a fee. Maternal healthcare is practically free of charge for those who qualify for the social benefits or have municipality of residents in Finland (EU- healthcare, 2021). When one is covered by the social insurance institution of Finland (Kela), those women are entitled to baby box, thus package for the baby and maternity allowances. In addition, maternal care is done at the maternal health clinics, university hospital and central hospitals. Education about safety of mother and baby is given, one is also offered an interpreter if there is a need, and all these are free of charge for EU members.
Furthermore, it is usually recommended that pregnant women visit the doctor in their fourth month of pregnancy, the doctor or more often midwife will then issue a certificate of pregnancy which the women can use to apply for social benefit and to give to their employer for maternity leaves. This strategy has motivated a lot of pregnant mothers to visit the antenatal clinics. One can also visit a private clinic, but it comes with a fee (Info. Finland, 2022). In Finland almost all childbirths are done at the hospital. Maternal mortality rates in Finland have been low as compared to the United States and has remained low. Comparing the maternal mortality in 2017 between Finland and United states, Finland had 3 deaths /100,000 live births while United States had 19 deaths /100,000 live births (WHO, 2019). However, foreign women have the highest maternal mortality rate in Finland as compared to the local people (Finnish Institute of Health and Welfare, 2022).
Fertility rate of foreigners in Finland.
According to Statistics Finland (2022), foreigners birth-rate increased from 10000 in 1990s and 12600 in 2020. The total fertility rate for foreigners was 1.7 in 2021, which is a bit higher than the fertility rate of 1.5 for the entire women population.
The diagram below shows the fertility rate of foreign women in Finland according to their various countries from 2000 to 2003 and 2018 to 2021 according to statistics Finland. From the figure 2 below, among foreign women in Finland, we can see that Somalis have the highest fertility rate among others. We can also see that fertility rate is reducing from 2018 -2021 except for women from Poland, Romania, and German women, whose fertility rate in Finland is increasing.
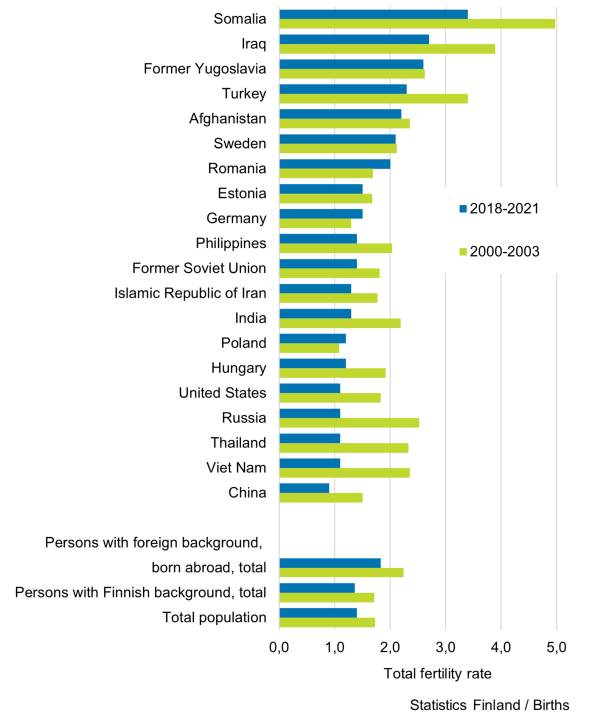
Figure 2; Fertility rate of foreign women in Finland. Source; (Statistics Finland, 2022).
Conclusion
Childbirth is very important for every family. Giving birth in a foreign country can have its positive and negative side. After going through various articles, it was found out that people go to different countries to give birth for citizenship, to benefit from low birth cost, quality health care, get social benefits, on the other side due to war and political instabilities, people migrate to different countries where they can find peace and stability to establish their family, but there are also challenges that comes with this. According to various studies some of these challenges for giving birth in a new country include, cultural differences, racism, insufficient knowledge in maternal healthcare, cost of healthcare and communication problems.
Moreover, going through the immigration process to get legal documents for the baby can sometimes be very stressful for foreigners since most countries do not grant permit or visa to babies automatically after childbirth. After reviewing several studies, it can be concluded that, before foreigners can achieve good quality maternal healthcare, all these challenges need to be addressed. Healthcare policy makers need to take into consideration foreigners when making policies to help solve cultural sensitivities, for example some developed countries have medicalized maternal care which may not help other cultures because in some cultures they believe in natural birth and may not need any pain medication or any other medications during childbirth but surprisingly they may be given these medications without even being informed.
Also, pregnant mothers with female genital mutilation may be considered for caesarean section birth without proper assessment whether they could have vaginal delivery, and this may be against their will. Furthermore, healthcare workers need to be educated on various cultures so they can apply it in the healthcare system to achieve good patient satisfaction. Moreover, patient education on their right to standard treatment, to know hospital policies and healthcare education should not be overlooked. There should be availability of language interpreters, phone interpreters and applications at all time and easy to access.
However, they are also good sides in giving birth in a foreign country, for example, some countries have universal healthcare system especially most Nordic countries like Finland, Norway, and Sweden, where almost everyone in the country have access to equal treatment, without any financial problems. Most people are also entitled to social benefits for both parents and the baby. Not forgetting the quality healthcare system and good human resources, modern and advanced technology to help in maternal healthcare. Also, comparing the maternal healthcare between Finland and America, one could see that institutional and government policies can greatly affect foreigners’ childbirth.
References
- American College of Obstetricians and Gynaecologists (2019). Levels of Maternal Care section b https://www.acog.org/Clinical-Guidance-and-Publications/Obstetric-Care-Consensus-Series/Levels-of-Maternal-Care?
- Ayers. S, Ford. E, (2007). Childbirth and Stress, Academic Press, Pages 467-471.
- Blais R, Maiga A, (1999). Do ethnic groups use health services like the majority of the population? A study from Québec, Canada. Social Science and Medicine, 48:1237-45
- Brar, S., Kale, M., Birch, C., Mattall. F., Vaza. M (2022) Impact of birth tourism on health care systems in Calgary, Alberta. BMC Health https://doi.org/10.1186/s12913-022-07522-4
- Chalmers, B. Omer-Hashi, K (2002). What Somali women say about giving birth in Canada. 10.1080/0264683021000033183. Journal of Reproductive and Infant Psychology - J reprod infant psychol.
- Chichirez, C. M., & Purcărea, V. L. (2018). Interpersonal communication in healthcare. Journal of medicine and life, 11(2), 119–122.
- EU- healthcare (2021). Pregnancy and Childbirth in Finland. Retrieved 15th August,2022). https://www.eu-healthcare.fi/healthcare-in-finland/special-treatment-situations-in-finland/pregnancy-and-childbirth-in-finland/
- Finnish institute of health and welfare (2022). Maternity Outcomes of Minority Women in Finland Survey (MOM) https://thl.fi/en/web/thlfi-en/research-and-development/research-and-projects/maternal-health-experiences-of-minority-women-in-finland-survey-mom-
- Garfield R, Orgera K, Damico A (2019). The Coverage Gap: Uninsured Poor Adults in States That Do Not Expand Medicaid. https://www.kff.org/medicaid/issue-brief/the-coverage-gap-uninsured-poor-adults-in-states-that-do-not-expand-medicaid.
- Griffith, A. (2018). An analysis of hospital financial data shows that birth tourism is rising, and not just in BC. The impact cannot be passed off as insignificant. Policy Options. https://policyoptions.irpp.org/magazines/november-2018/hospital-stats-show-birth-tourism-rising-in-major-cities/
- Higginbottom, G., Morgan, M., Alexandre, M., Chiu, Y., Forgeron, J., Kocay, D., & Barolia, R. (2015). Immigrant women’s experiences of maternity-care services in Canada: a systematic review using a narrative synthesis. Systematic reviews, 4(1), 1-30.
- Hill, N., Hunt, E., & Hyrkäs, K. (2012). Somali immigrant women's health care experiences and beliefs regarding pregnancy and birth in the United States. Journal of transcultural nursing: official journal of the Transcultural Nursing Society, 23(1), 72–81
- Info. Finland (2022). When a child is born in Finland. https://www.infofinland.fi/en/family/children/when-a-child-is-born-in-finland.
- Janevic, T., Sripad, P., Bradley, E., & Dimitrievska, V. (2011). "There's no kind of respect here" A qualitative study of racism and access to maternal health care among Romani women in the Balkans. International journal for equity in health, 10, 53. https://doi.org/10.1186/1475-9276-10-53
- Jarvis C, D’Souza V, Graves L. (2019) Uninsured Pregnant Patients: Where do we Begin? Obstet Gynaecol;– https://doi.org/10.1016/j.jogc.2018.10
- Malin, M., & Gissler, M. (2009). Maternal care and birth outcomes among ethnic minority women in Finland. BMC public health, 9, 84. https://doi.org/10.1186/1471-2458-9-84
- Mehrara. L, Karine. T Gjernes. O & Young. S, (2022) Immigrant women’s experiences with Norwegian maternal health services: implications for policy and practice, International Journal of Qualitative Studies on Health, and Well-being, 17:1, 2066256, DOI: 10.1080/17482631.2022.2066256
- Mieli (2021) immigration. Retrieved on 10th August 2022. https://mieli.fi/en/difficult-situations-in-life/immigration/
- Montreal., (2011). Measuring racism: cutting edge work of the CDC Racism and Health Working Group. Annual Meeting of the Society for Epidemiologic Research.
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Division of Behavioural and Social Sciences and Education; Board on Children, Youth, and Families; Committee on Assessing Health Outcomes by Birth Settings; Backes EP, Scrimshaw SC, editors (2020) Birth Settings in America: Outcomes, Quality, Access, and Choice. Washington (DC): National Academies Press (US) Maternal and New-born Care in the United States. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555484/
- National Center for Health Statistics (2021). Natality public-use file and CD-ROM. Hyattsville, MD
- PRB (2003). U.S. fertility rate higher among minorities. https://www.prb.org/resources/u-s-fertility-rates-higher-among-minorities/
- Quagliata, E. (2013). Becoming parents and overcoming obstacles: Understanding the experience of miscarriage, premature births, infertility, and postnatal depression. Taylor & Francis Group.
- Schiff, M. (Ed.). (2007). International migration, economic development & policy. World Bank Publications.
- Singh G. K. (2021). Trends and Social Inequalities in Maternal Mortality in the United States, 1969-2018. International journal of MCH and AIDS, 10(1), 29–42. https://doi.org/10.21106/ijma.444
- #Statistics Finland (2022). Birth rate. Retrieved 20/9/2022. https://www.stat.fi/tup/maahanmuutto/perheet/syntyvyys_en.html
- The Guardian News (2020), The reverse birth tourists: US women seek cheaper countries to have babies Retrieved 10th August 2022. https://www.theguardian.com/us-news/2020/aug/07/reverse-birth-tourists-americans-are-having-babies-abroad
- Triebwasser JE, Kamdar N, Moniz MH, Langen ES (2018). Journal of the American Medical Association. Smith J, Morgan RD, Morgan DM. Hospital contribution to variation in rates of vaginal birth after caesarean: A Michigan Value Collaborative study. American Journal of Obstetrics and Gynecology. ;218(1): S351–S352.
- World Health Organization (2019). Trends in maternal mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: Executive summary. Geneva, Switzerland: World Health Organization
- World health organization (2022) Quality care. Retrieved 1/09/2022.https://www.who.int/health-topics/quality-of-care.
- World health organization (2022). Female genital mutilation. Retrieved 13th October 2022. https://www.who.int/news-room/fact-sheets/detail/female-genital-mutilation.